Lumbar disc herniation
What causes disc herniation in the lumbar region?
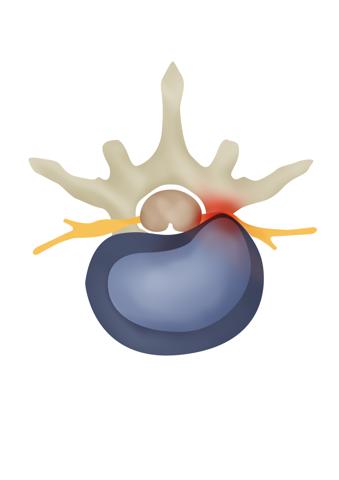
Lumbar disc herniation is closely related to the structure of the disc. The intervertebral disc consists of two parts – a dense circular ring that contains a thick gel-like core. The intravertebral discs are essential and important structures functioning as shock absorbers (provide cushioning between the vertebrae), they are integral for maintaining posture and permitting a wide degree of movement, they also provide support to the adjacent vertebrae of the spine
A disc hernia forms when the outer ring of the intervertebral disc ruptures and the core inside the disk ring protrudes through the rupture site outside the ring. Symptoms of intervertebral disc herniation present themselves when the nucleus of the disk protrudes in the vicinity of, or directly into an adjacent nerve. Complaints are therefore tied to the innervation region of the affected nerve (in the case of the lumbar spine – all nerves descend and innervate the legs. Sometimes the herniation happens in a direction that does not come in contact with any nerves, in such a case lumbar disc herniation can be completely asymptomatic.
Disc protrusion is an often finding on radiological examinations. Unlike in the case of a disc hernia, in the case of disc protrusion the structural integrity of the disc itself is preserved, it is instead deformed or dislocated. Small/insignificant disc protrusions are seen in almost every examination (magnetic resonance imaging or computed tomography), but they seldom cause symptoms. It is, however, possible for a disc protrusion to be large enough to depress an adjacent nerve and trigger the corresponding nerve impingement symptoms.

What are the factors that increase the risk of developing a disc herniation?
Intervertebral disc herniation is a common disease. It mainly affects individuals between the ages of 25 and 50. Men get this disease about two times more often than women. Heavy physical labor increases the risk of both the illness and its recurrence. Not only does increased body weight significantly increase the risk of developing a disk hernia, it also increases the risk of disk hernia recurrence, and furthermore, increases the risk of redeveloping a disc hernia by approximately 12 times in patients who have undergone a microdiscectomy operation.
Smoking (nicotine) reduces the blood supply to the intervertebral disc, which in turn contributes to the degeneration of the disc (worsening and aging of cellular functions) and delays its healing.
Of course, disk hernia can occur in anyone and at any age, and for no known reason.
Symptoms of disc herniation tend to occur for no discernible reason, but sometimes it is associated with lifting weights, clumsy turning, pushing or pulling. As the pressure and load on the spine increases, especially in people with weak and poorly developed postural muscles, the disc may puncture, burst, or rupture, which in turn may have an effect on the adjacent nerve root that directs impulses to the foot. The result is severe shooting pain in the buttocks and leg.
What could be the symptoms of lumbar disc herniation?
- Leg pain (radicular leg pain aka sciatica) This pain is usually much more severe than back pain. The pain may be sharp, shooting, persisting.
- Back pain. May be encountered in the early stages of the disease.. If the pain is experienced, it is usually much less expressed than leg pain.
- Tingling and/or numbness in the leg, observed less commonly in both legs.
- The localization of pain and numbness depends on the level at which the disc herniation is located (between which vertebrae). Symptoms may manifest themselves in the buttocks; front or back of thigh; lower leg; front, back or side of the leg; at the foot. Symptoms are commonly present in only one leg.
- Pain is provoked by movement. Patients will complain of pain exacerbation after lengthy sitting, standing or walking a short distance. Sneezing, coughing and laughing can oftentimes cause severe pain.
- Muscle weakness. Dangerous symptom showing a very strong nerve compression.[UR1]
- Urinary disorders (urinary incontinence, painless or painful urinary retention) and defecation disorders, saddle anesthesia (?) and weakness in both legs are rare (1% to 2% of disc herniated operations) but very dangerous symptoms. Medically it is called equine (many nerves of the lumbar and sacral region) compression (impingement) syndrome. In the case of major disc herniation and equine compression syndrome there is a very high risk, about 45%, that even after a successfully performed decompression surgery some dysfunction of urinary and/or bowel continence and sexual function can persist.[UR2]
- [UR1]Sugg. Red flag symptom?
- [UR2]There is an elevated risk (approximately 45%), that even in the case of a completely successful decompression surgery some urine or bowel dysfunction can persist, sexual function may also be affected.
What examinations are needed?
If you have any of the symptoms described above, you should first see your doctor. A detailed patient history and neurological examination is often sufficient to narrow down the physicians’ suspicion to the exact level of the lesion, it is thereafter possible to precisely target this region when MRI/CT investigations are carried out. These investigations will prove just as useful in younger patients with normal body weight, presenting with suspicions of a disc hernia. A timely consultation will save time and avoid unnecessary investigations, as well as save you some trouble and concern as what to expect from this disease.
In case there is a need for our specialist opinion, we are happy to help. We provide appointments and consultations for both – residents of Latvia and patients from abroad, including remote appointments via video-call. There are a number of ways to schedule appointment with one of our specialists, electronically (for Latvian residents) or requesting a remote appointment via video call by email or through the telephone contact.
What are the treatment options?
Treatment options are discussed and decided upon with the help of your physician. If your complaints, neurological status, and radiological findings are consistent with your initial conservative (non-operative) treatment goals, your doctor will inform you about the current treatment plan and any changes made and also plan your next follow-up visit. In case of severe pain, you may be offered invasive analgesic (pain injections)-epidural steriod injection.
In what cases disc herniation surgery should be performed?
In the case of symptomatic lumbar disc herniation, surgery will be required only in 10-20% of patients.
An operation is performed on elective basis if:
- Pain and other symptoms persist after 6 weeks of comprehensive conservative therapy;
- An operation is performed on urgent/semi-urgent basis if:
- The patient suffers from severe pain that cannot be alleviated by medications or blockades, and this pain results in severely limited daily activities such as walking, standing;
- Neurological symptoms (weakness and / or numbness of the leg) progress (worsen);
- Urinary and/or bowel incontinence, sexual dysfunction occurs.
What does surgery mean in case of this disease?
The most common operation performed on a lumbar disc herniation is microdiscectomy. It is a minimally invasive surgery that is performed through a 2.5-3 cm incision. An X-ray machine is used for precision guidance and additional patient safety, both before and during surgery. The surgery is performed under microscope control, the disc fragments are removed from the herniated region and the affected nerve/s are decompressed. The intervertebral disc is a very important and integral structure of the spine, that’s why the aim of this surgery is to remove the herniation while preserving as much of the disc as possible.
Patients only need to spend one night at the hospital after the operation, the next morning a physiotherapist is there to help them to get up and start exercising, after that the patient is released to go home. It takes 3-4 weeks after surgery to resume normal daily activities and return to work.
We provide world class neurosurgical treatment for Latvian residents and for international patients. Learn more here if you are international patient considering having treatment with us.
The venue for surgical interventions is perfectly equipped private hospital in Riga – “Aiwa clinic”.
What regimen should I to follow after disc herniation surgery?
Because the greatest pressure on the disc develops while the person is sitting, leaning forward and lifting weights, the following regimen of 3-4 weeks after surgery should be followed to prevent a disc herniation from recurring:
- do not sit – avoid sitting positions as much as possible. The patient is free to stand, walk and sleep but not sit! Even getting up from bed should be done in such a way as to avoid sitting up. Getting up from bed and specific physical exercises that are recommended after regular surgery will be taught to you by a physiotherapist on the first day after surgery.
- Do not bend forward – bending forward increases the pressure on the disk, thus increasing the risk of re-herniating a disk and should therefore be avoided. After the surgery, the physiotherapist will teach you how to properly lift objects from the ground without bending forward.
- Do not lift weights – lifting weights increases the pressure on the intervertebral disc and thus increases the risk of re-herniating the disc and should be avoided.
- Do not twist your body- twisting of the spine can increase the risk of re-herniating a disc and should therefore be avoided.
What are the results of lumbar disc herniation surgery?
Microdiscectomy is a very effective operation with good and excellent results in 84-90% of cases. Results are the disappearance of neurological symptoms (pain, numbness, muscle weakness in the leg). Lumbar microdiscectomy is not effective in treating low back pain. This operation is not performed if back pain is the main complaint.
Microdiscectomy is considered a low-risk operation, but every invasive manipulation has its risks. Recurrence of a disk hernia at the same localization is the most common problem. This occurs most often during the first three months after the surgery. The instructions of your doctor and physiotherapist should be strictly followed to avoid recurrence of disc herniation.
ou can learn more about experience of our international and Latvian patients by checking testimonials page.